 THE CAURA PALLIATIVE CARE UNIT
THE CAURA PALLIATIVE CARE UNIT
Tel 662-4053
What is Palliative Care?
- Palliative Care is the total care of patients whose disease is not responsive to curative treatment
- Control of pain and other physical and psychosocial problems is paramount
- Affirms life and regards dying as a normal process
- Intends neither to hasten nor promote death
- The goal of palliative care is achievement of the best possible quality of life for patients and their families.

The Caura Palliative Care Unit (PCU)
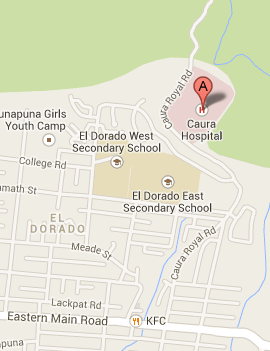
The Caura Palliative Care Unit is a 12-bed inpatient unit situated on the grounds of the Caura Hospital in El Dorado. This Unit was a joint initiative between the North Central Regional Health Authority(NCRHA) and the Palliative Care Society of Trinidad and Tobago (PCSTT). The PCSTT is a not for profit organization started by Mr. and Mrs. Satyernand Seemungal, in honour of their daughter Trudy-Ann Seemungal-Velauytham, who passed away from cancer and to whom the Unit is dedicated. The Unit opened its doors on August 5th 2014.
Aims of the Caura Palliative Care Unit
- To provide relief from pain and other physical symptoms
- To maximize quality of life
- To provide psychosocial and spiritual care
- To provide support to the family during the patient’s illness and in their bereavement
Section I
INFORMATION FOR FAMILIES
ADULT SERVICE
What can we help with?
Referrals are accepted for adult patients (over age 18) with a diagnosis of an advanced, progressive, life-limiting illness and complex specialist palliative care needs.
Many of our clients will be patients with advanced cancer, but those with other conditions such as advanced organ failure (e.g. heart failure, kidney or liver failure) are also cared for.
Complex needs requiring admission could be severe pain, bowel obstruction, dependence on oxygen, inability to swallow medication to control symptoms and difficult wounds, among others.
 In-Patient Service
In-Patient Service

Our Unit has a capacity of 12 beds, and patients are admitted for one of three reasons:
- Control of symptoms
- Care at the end of life
- To provide respite for the family/caregiver
OUR TEAM
We have a dedicated team of nurses, doctors, social workers and psychologists, domestic and kitchen staff and volunteer chaplains, all of whom are here to support you and your family.
QUICK FACTS
- We encourage you to spend time with your loved one. Unfortunately, due to Covid-19, we have had to restrict visitors to protect our vulnerable patients. Visiting regulations vary depending on risk, so the team will update you on the current regulations.
- We ask that visitors please observe infection control protocols such as not visiting if you are feeling unwell, washing hands on entering and leaving the patient’s bedside, wearing a properly fitting mask that covers the nose and mouth if you have respiratory symptoms and not congregating in the hallways or patient bays.
- Please be forewarned that visiting might be interrupted by activities such as tidying of patients and patient rest periods. The nurse in charge can take a decision to restrict visiting, if it in deemed in the patient’s best interest. If your loved one is agitated, as often happens at the end of life, we recommend a quiet environment, with noise and stimulation kept to a minimum.
- All our rooms are shared, so we ask visitors to please be sensitive to the needs and privacy of the other patients in the room.
- We suggest that family members coordinate and schedule the visiting so that the patient has someone with him as much as desired and one person does not get burnt out.
- One relative is allowed to stay overnight in the recliner next to the patient’s bed. This is not mandatory and may be more necessary for agitated patients who need to see a familiar face to re-orient them. Please check with the nurse in charge if you are interested in staying overnight.
- We kindly ask family members and all visitors to adhere to Caura Hospital’s dress code which is posted on the wall in the main hospital entrance. We ask that persons permitted to stay overnight on the ward observe modesty in dress. Comfortable lounge wear like track pants and t-shirts are preferred for overnight stay for women.
- The hospital’s gates are locked at 8pm to ensure the safety of patients and staff. Should you have special circumstances that require later visiting, please talk with a member of our nursing staff to arrange.
- We recognize that this can be a very stressful time. If you feel that you need support e.g. counselling or other assistance from our chaplain or social worker, please let our team know as early possible.
SHARING OF INFORMATION
Our team is here to protect the patient’s best interest. We will therefore share medical information only with the person designated as next-of-kin by the patient, the person having legal power of attorney, the nearest blood relative or other designated relative. If there are important decisions to be made, we would invite family members for a meeting, so that we do not have to repeat information.
LEGAL MATTERS
We advise families to ensure that legal matters are dealt with as early as possible, preferably before admission to the Unit, as some patients decline rapidly, becoming unable to participate in decision-making.
Should wills or other legal documents need to be drawn up while the patient is on the Unit, we advise families to arrange their own legal counsel and psychiatrist (if mental capacity needs to be assessed). The legal department of the NCRHA has advised our health care team NOT to be involved in these personal legal matters.
CPR (CARDIOPULMONARY RESUSCITATION)
Our patients all have very advanced diseases that are beyond cure. Our goal of care is to help improve symptoms and ensure better quality of life. In keeping with this goal, we do not recommend CPR for our patients.
CPR is most successful when performed immediately, in relatively healthy persons who have had a witnessed cardiac arrest. For our patients, who are the end stage of cancer of organ failure, CPR is usually futile and if the heart does start pumping again, the patient will usually be in a poorer condition after being deprived of oxygen during the arrest.
Should a patients’ heart or lung stop functioning, we will provide oxygen and other interventions to ensure comfort, we will allow family members to be present and religious rites to be complete and we will do everything to ensure a dignified passing.
ARTIFICIAL NUTRITION AND HYDRATION
For patients at the end of life, artificial feeding is not usually appropriate. Fluid given into the veins (commonly referred to as drips), can cause swelling of the limbs and body and can even cause fluid to accumulate in the lungs of very sick patients. Tubes placed through the nose into the stomach for feeding are unpleasant and are rarely used in patients close to death, when we want to minimize distress. These patients will be encouraged to take as much as they safely can by mouth. In many cases the patients safely tolerate chips of ice, sips of liquids or syringe feeds.
Intravenous fluids and feeding tubes are therefore rarely indicated for our patients.
FUNERAL HOME
The Caura Hospital has no mortuary facilities. We therefore need families to choose a funeral home, to complete the funeral home form in the admission package and to return it to the nursing staff as soon as possible after the patient is admitted. We recognize that this may be unpleasant and that some persons are not comfortable thinking about their loved one passing away, but we need to have a funeral home documented on file for all admissions.
Should your relative pass away without completion of the funeral home form, a funeral home of the Regional Health Authority’s choice will be contacted and any expenses incurred will be passed on to the family. This system is necessary to ensure that deceased persons are removed promptly, avoiding distress to other patients in the room.
DISCHARGE FROM THE UNIT
The Unit at Caura is a specialist unit, with only twelve beds. We are therefore unable to accommodate patients for long term care. Should your loved one improve significantly so that he/she no longer requires specialist care, we would recommend discharge home or transfer to a longer-term facility. We realize that many families are happy with our care and would prefer their relatives to stay here, but we are unfortunately not able to facilitate this.
Once discharged, patients can be readmitted if complicated symptoms return. We hope that you will understand our need to reserve our beds for those with the most difficult symptoms and the greatest need.
If we are discussing discharge with you, it is because your loved one is doing much better than expected.
Please be assured that there will be no sudden discharge. You will be involved in the process of discharge planning and the Social Worker’s help will be sought, if necessary, to arrange the best place of care.
- Out-Patient Service
Out-patient clinics are held on Mondays and Wednesdays at the Unit, from 8 am to 1pm and are by appointment. Most of our follow-up appointments are done by telephone to avoid patients having to come to the hospital.
For new patients and patients with new symptoms who need urgent assessment, in person visits are still offered.
In order to optimize your time, please try to arrive fifteen minutes before your scheduled appointment. Each appointment can last for up to an hour. If you are unable to make an appointment, please call the unit on 662-4053 to reschedule.
At the clinic, our team discusses:
- The patient’s symptoms
- The patient’s care and options for care
- Plans for the future
At the end of the clinic we provide you with a copy of an agreed upon plan of action, as well as a prescription for medication, most of which are available from our inpatient Pharmacy.
We continue to provide support via phone for out-patients to address the following:
- Symptoms not well controlled at home
- Concerns about a change in the patient’s medical condition
- Queries about the medicine dose
- Reports of side effects of medicine
- Caregiver support
Unfortunately, our service cannot provide support for:
- Unplanned admissions
- Emergencies/Trauma
- Procedures e.g. blood transfusions, chest/abdomen drains or taps, insertion of feeding tubes etc.
- Provision of anti-cancer medication or interventions such as chemotherapy and radiotherapy.
PAEDIATRIC SERVICE
The WHO defines palliative care for children as the active total care of body, mind and spirit and also involves giving support to their families.
Since 2022, the Caura PCU has been providing services to Paediatric patients under the care of Paediatric Palliative Care Specialist, Dr Elizabeth Persad.
Unfortunately the PCU is not yet able to provide out-patient clinic or inpatient admission for children at the Caura hospital. The service currently comprises consultations at EWMSC and tele-heath follow-up of referred children and their families.
SHOULD YOU HAVE ANY QUESTIONS ABOUT OUR SERVICE OR POLICIES, please feel free to speak with any member of the medical or nursing team.
IF YOU HAVE ANY COMPLAINTS OR CONCERNS, please communicate with either of the following:
Head Nurse or Lead Physician on 662-4053
We look forward to working together during this challenging time to provide the best possible care for you and your loved one.
Section I
INFORMATION FOR HEALTH PROFESSIONALS
ADULT SERVICE
WHO SHOULD BE REFERRED
Adult patients (over 18 years old), with life-limiting illnesses* who have any of the following:
- Complex physical symptoms (e.g. dyspnoea and oxygen dependence, pain, GI bleeding, constipation, inoperable bowel obstruction, agitation etc) which need specialist management.
- Complex psychological issues (depression, denial, maladaptive coping etc), which need specialist management.
- Patient in the terminal phase, with a prognosis of days to short weeks, stable enough for transfer, who require admission for end-of-life care.
*A life-limiting illness is one where it is expected that death will be a direct consequence of the specified illness e.g. advanced cancer, end-stage heart, lung, renal disease etc.
PATIENTS WHO ARE UNLIKELY TO BE APPROPRIATE*
*Please call to discuss if necessary
- Patients with poor social support who happen to have stable cancer/other medical conditions but NO complex symptoms. These would be better served by referral to Social Work. We unfortunately cannot accommodate socially displaced, stable patients.
- Patients likely to die before transfer and who have no complex symptoms. Do call if symptom control advice would be helpful.
- Stable CVA/Dementia/neurological diseases or persistent vegetative state patients who are still being PEG/NG fed and require long term care.
IN-PATIENT vs OUT-PATIENT
- Patients with acute distressing symptoms unfit for transfer or outpatient clinic, should be referred for in-patient Our hospital consult service is limited but we will try to facilitate for appropriate patients with refractory symptoms. This service is limited to two institutions of the NCRHA: the Eric Williams Medical Sciences Complex and the Women’s Hospital.
- Patients with stable or mild symptoms who are ambulant or easily conveyed by wheel-chair can be referred to our out-patient
- Patients who are bed bound, or have depressed conscious levels are not appropriate for out-patient referral and may need to be referred for admission.
BEFORE REFERRING
- Please ensure that patient & family have been told the diagnosis and understand that it will shorten the patient’s life.
- Please ensure that patient & family understand what palliative care means and that they agree to the referral.
- Please talk to family about preferences for place of care and explore their support system. It is not necessary for us to review at EWMSC if home is the preferred place of care and family support is good. Out-patient clinic review or an out-patient family meeting can be arranged to discuss future care options.
- Please call the Unit if there are any doubts as to the appropriateness of the referral or if you consider it urgent.
PAEDIATRIC SERVICE
The WHO defines palliative care for children as the active total care of body, mind and spirit and also involves giving support to their families.
WHO SHOULD BE REFERRED
Referral is appropriate once a child is diagnosed with a life limiting or life threatening illness in any of the following categories, even if the child is not yet born:
- Life threatening conditions e.g. cancer, organ failure and long term ventilation
- Conditions in which premature death is inevitable e.g. Duchenne’s and cystic fibrosis.
- Progressive conditions without curative treatment options e.g. metabolic conditions and incurable cancer
- Irreversible, non-progressive conditions e.g. severe cerebral palsy, brain or spinal cord injury
TO REFER TO OUR ADULT OR PAEDIATRIC SERVICE
Please complete all sections of one of our referral forms.
For Out-patient referrals
If this is a non-urgent referral, the form can be given to patient/family and they can call the Unit (Tel: 662-4053) between 8am and 4pm to make an appointment. Alternatively the form can be sent to our team via what’s app on 339-6265 by either the referring doctor or the family member. Please ensure that the referral form is completely filled in.
For urgent referrals (which need to be seen within 1 week), please contact a member of our team to discuss and to arrange an early appointment
For In-Patient review (only available at EWMSC & Mt. Hope Women’s Hospital)
Please contact us on 662-4053 to explain the need. The referral form can be left in the patient’s file.
Please ensure that referred in-patients remain under your team’s care while awaiting our review. As an off-site team we cannot take responsibility for “discharged” patients who remain on the ward.
There is no emergency department or out of hours service at Caura hospital. All admissions and clinic appointments must be pre-arranged. Please do not direct families to bring patients to Caura straight from wards, emergency rooms, or clinics in the hope of being seen. Urgent reviews must be arranged with a member of our team.
Thank you for your support in ensuring that our service runs efficiently, and provides the best care for those most in need.
Caura Hospital Palliative Care Unit
Caura Hospital,Caura Royal Road, El Dorado,Trinidad. Phone: 662-4053
REFERRAL FORM FOR PALLIATIVE CARE
NAME: DOB: AGE:
ADDRESS: GENDER: MALE/FEMALE
CURRENT LOCATION: HOME/HOSPITAL/OTHER
MAIN CARE-GIVER/NEXT OF KIN
NAME: RELATIONSHIP:
ADDRESS: PHONE NUMBER:
DIAGNOSIS & CURRENT CONDITION:
| MAIN DIAGNOSIS: | DIAGNOSIS BASED ON HISTOLOGY/RADIOLOGY/CLINICAL FINDNGS DETAILS:
|
| SITE OF METASTASES: | OTHER DIAGNOSES:
|
| CURRENT CONDITION: STABLE/IMPROVING/DETERIORATING
ABLE TO TOLERATE ORAL FEEDS YES/NO NGT/PEG FOR FEEDING YES/NO TRACHEOSTOMY YES/NO (We are currently unable to accept patients with tracheostomies for admission) | |
| MEDICATION:
| |
Please call our team on 662-4053 to discuss all referrals, both for admission and out-patient clinic. Please do not send any patients directly to the Unit without prior discussion with our team as we have limited beds and no emergency service.
REASON FOR REFERRAL (Please circle or tick & give details)
IN-PATIENT ADMISSION OUT-PATIENT CLINIC
| SYMPTOM MANAGEMENT (Complex acute symptoms requiring in-patient care) |
|
| END-OF-LIFE CARE (Poor performance status and estimated prognosis of days to short weeks maximum) |
|
| RESPITE (Max 2 week admission in case of caregiver burnout or need to improve home care package) |
|
ECOG PERFORMANCE STATUS (Please circle)
| 1 | Ambulatory & able to carry out light work |
| 2 | Ambulatory & capable of all self-care but unable to carry out work activities. Up and about more than 50% waking hours |
| 3 | Capable of only limited self-care, confined to bed/chair more than 50% waking hours |
| 4 | Completely disabled, cannot carry out any self-care |
PROGNOSIS (Please circle): DAYS WEEKS MONTHS
Please indicate the urgency of this assessment (Please circle)
EMERGENCY (needs to be seen within 24hours)
URGENT (needs to be seen within 1 week)
NON-URGENT (within 2-4weeks)
*PLEASE ENSURE THAT THE FOLLOWING CRITERIA ARE MET PRIOR TO REFERRAL
| Patient & family informed of diagnosis & agree to referral to Palliative Care | Yes/No |
| CPR has been discussed with patient or family | Yes/No |
| In cases of no family support, a referral has been made to Social Work | Yes/No |
| Consultant had deemed patient appropriate for Palliative care | Yes/No |
| Name of Consultant(s) making the decision: | |
Name of referring doctor_______________________________________________________________
Signature______________________________Date:_________________________________________
Contact Number_______________________ Consultant _____________________________________
